- Created by Ian Green, last modified on 2023-Mar-23
Group name
Eye Care CRG
Date
23rd, March 2023 at 12.30 - 14.00 UTC
Attendees
- Anthony Khawaja Ian Rodrigues Elaine Wooler Ian Green Joshua Stein, Benjamin Zu Cindy Cai Sally Baxter
Apologies
Recording (GoogleDrive)
https://drive.google.com/file/d/1Jx_Zl1x6RIe3c-uZoWWgSiJRUsovenbU/view?usp=share_link
Discussion items
| Item | Description | Owner | Notes | Action |
|---|---|---|---|---|
| 1 | Welcome and apologies | Anthony | ||
| 2 | Update from diagnoses/procedures group | |||
| 3 | Discussion | |||
| 4 | Updates from Findings/signs group | |||
| 5 | Discussion | |||
| 6 | Questions from members, users, SNOMED authors | |||
| 7 | Other items | |||
| 8 | Next meeting |
|
Meeting Files
| File | Modified | |
|---|---|---|
| Microsoft Powerpoint Presentation SNOMED Eye Care CRG – Update on Glaucoma_FINAL.pptx | 2023-Mar-22 by Ian Rodrigues | |
|
Labels
|
||
| PDF File Glaucoma Preferred SNOMED Terms_March 2023.pdf | 2023-Mar-22 by Ian Rodrigues | |
|
Labels
|
||
| Microsoft Excel Spreadsheet Glaucoma concepts Jan 2023 International release.xlsx | 2023-Mar-22 by Elaine Wooler | |
|
Labels
|
||
| Microsoft Powerpoint Presentation Gaps in Glaucoma Exam Findings 2023 03 23.pptx | 2023-Mar-23 by Sally Baxter | |
|
Labels
|
||
| PDF File Glaucoma diagnoses action points.pdf | 2023-Mar-23 by Ian Rodrigues | |
|
Labels
|
||
| PNG File image-2023-3-24_20-5-55.png | 2023-Mar-24 by Ian Rodrigues | |
|
Labels
|
||
| PNG File image-2023-3-25_20-12-41.png | 2023-Mar-25 by Alejandro Lopez Osornio | |
|
Labels
|
||
{kind=link}
{kind=link}
Previous Meetings
| Title | Creator | Modified |
|---|---|---|
| No content found. | ||
- No labels
9 Comments
Sally Baxter
Hi Elaine Wooler Can you advise me on where would be best to post the list of IOP modifiers and gonioscopic exam data elements, as we discussed in the meeting today? I wasn't sure if I should create a new discussion thread for each topic on the "Discussions" page? Or, should I create a document that I then upload here as a meeting file attachment? (I already uploaded the slide deck as a reference.) I am happy to follow whatever works best with your normal workflows. Also, my apologies, but it's almost midnight in my local time zone (currently based in Japan), and I will be out on spring break with my kids starting tomorrow, so I won't be able to post the information until I get back, but I figured I'd ask how best to present the information (or where to put it on Confluence) so I can do that when I return. My apologies for forgetting to ask this during the meeting today, but thank you for your help!
Elaine Wooler
Hi Sally Baxter probably best as a discussion item and then we can comment as needed. Thanks for this.
Ian Rodrigues
Action points for the glaucoma diagnoses work uploaded - sorry Elaine Wooler - they will mostly require your input!
Eric Brown
FYI, the UMLS metathesaurus browser is another great resource to find what vocabularies have certain terms (in many languages.) The page for "angle closure glaucoma" (https://uts.nlm.nih.gov/uts/umls/concept/C0017605) lists 181 atoms including a SNOMED synonym of "Narrow cleft glaucoma" which I don't remember encountering before.
Eric Brown
Sorry about missing the meeting this morning (and this long comment). I was actually seeing someone with an acute exacerbation of (likely) chronic angle closure glaucoma (did I get that wording right even though everyone else who has seen this gentleman called it "acute angle closure glaucoma"?) I watched the video (thanks Sally) this afternoon.
For my 2 cents, to be useful I'd suspect that laterality needs to be pre-coordinated and built into each code. It's not uncommon for patients to have 2 different severities or even causes of glaucoma in each eye, and so the history of the diseases of each eye needs to be well specified.
If, for example, we wanted to see whether anti-VEGF injections led to glaucoma, we'd need to be sure that the eye which got the anti-VEGF injections is the same one that has glaucoma of a certain severity. Without a clear, unambiguous way to tell that OD has X and OS has Y, correlations between exposures (systemic, OD, OS, or OU) and glaucoma will be error-prone to determine. Similarly, I'm sure we've all had patients who've had NVG which severely affected one eye but was recognized early enough to not affect the other. Without baking in laterality (or having it somehow intimately tied to the SNOMED code for the disease), it would be hard to use population data to try and determine what intervention gives the best outcome.
So I'd be in favor of having OD, OS, OU, unspecified for each disease state or finding. If there's a separate code for severity (mild, moderate, severe, unspecified, indeterminate) which also has a laterality (so 4x4 = 16 codes) then perhaps each disease state wouldn't need an additional layer of severity in addition to the laterality.
Anthony Khawaja
Thanks Eric. This again comes down to pre vs post co-ordination. While I always thought post- would be better, so we can be more parsimonious with the number of terms (as a coder, I hate the inefficiency / redundancy of pre-coordination - post co-ordination is so much more elegant), perhaps we will never get full agreement on this. Maybe we do just have OD, OS, OU, unspecified as more granular terms under all our diagnoses? But what about severity - are we happy to keep that post co-ordinated? As you 4x4 is starting to get really unpalatable for neat-freaks like me!
Eric Brown
Yes, I too hate inefficiency and redundancy. For many questions of academic interest, though, I don't care whether the person has glaucoma as much as whether the eye has glaucoma (many of my treatments treat the eye, not the patient systemically). On the other hand, each eye can only have 1 level of severity in its glaucoma disease. I think that Joshua Stein in the meeting had the question about whether there could be a separate set of concepts for the severity.
So, each eye could have two somewhat independent codes. For example, an individual could have "neovascular glaucoma, right eye", "primary open angle glaucoma, left eye", "severe glaucoma, right eye", and "mild glaucoma, left eye". With those 4 concepts it would be easy to tell that the right eye was severely affected by neovascular glaucoma and the left eye was mildly affected by POAG. But it wouldn't require adding 16 additional classes for each glaucoma diagnosis (only 4 for the set of eyes: OU, OD, OS, ??).
I was hoping that this might be a happy medium between pre-coordination and no-coordination(?)---because without making it unambiguous which eye has which condition at what severity, the coding system will be under-specified and less useful to communicate an actual person's health state and history.
Ian Rodrigues
Thanks Eric Brown you make some excellent points and I think the above would be a pragmatic solution - to have right / left / bilateral versions of diagnoses.
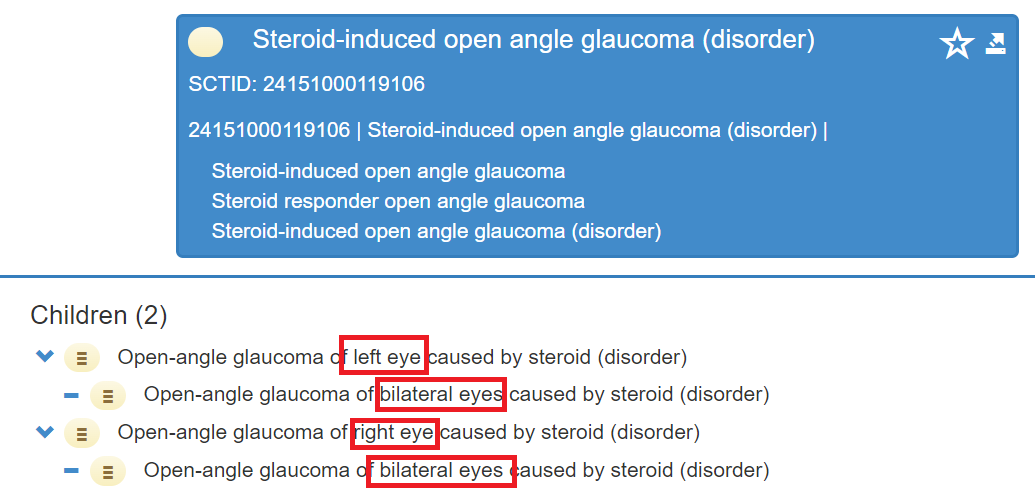
In SNOMED terms, I think the "Steroid induced open angle glaucoma" would be a good model to follow where the right and left eye versions are children/descendants of the no laterality specified code and the bilateral version is a child/descendant of the right and left eye versions:
If this is agreed on, perhaps these can be applied to the list of preferred diagnoses terms for glaucoma only (once we finalise them) and then applied in the same manner to any new glaucoma diagnoses codes that are approved.
I suspect that the EMRs (the ophthalmology specific ones at least) would elect to continue to limit the user facing diagnosis list to the ones with no laterality specified and capture the laterality in the standard way that is used in their systems, but this would enable an opportunity to then map this back to the appropriate SNOMED code with the appropriate laterality.
I agree that if we create a set of severity qualifier codes that also include laterality version as you suggest this would then work well. It may well be that these are not necessarily SNOMED (disorder) codes, but could be SNOMED (staging scale) or (situation) codes depending on what Elaine Wooler and her colleagues advise?
Alejandro Lopez Osornio
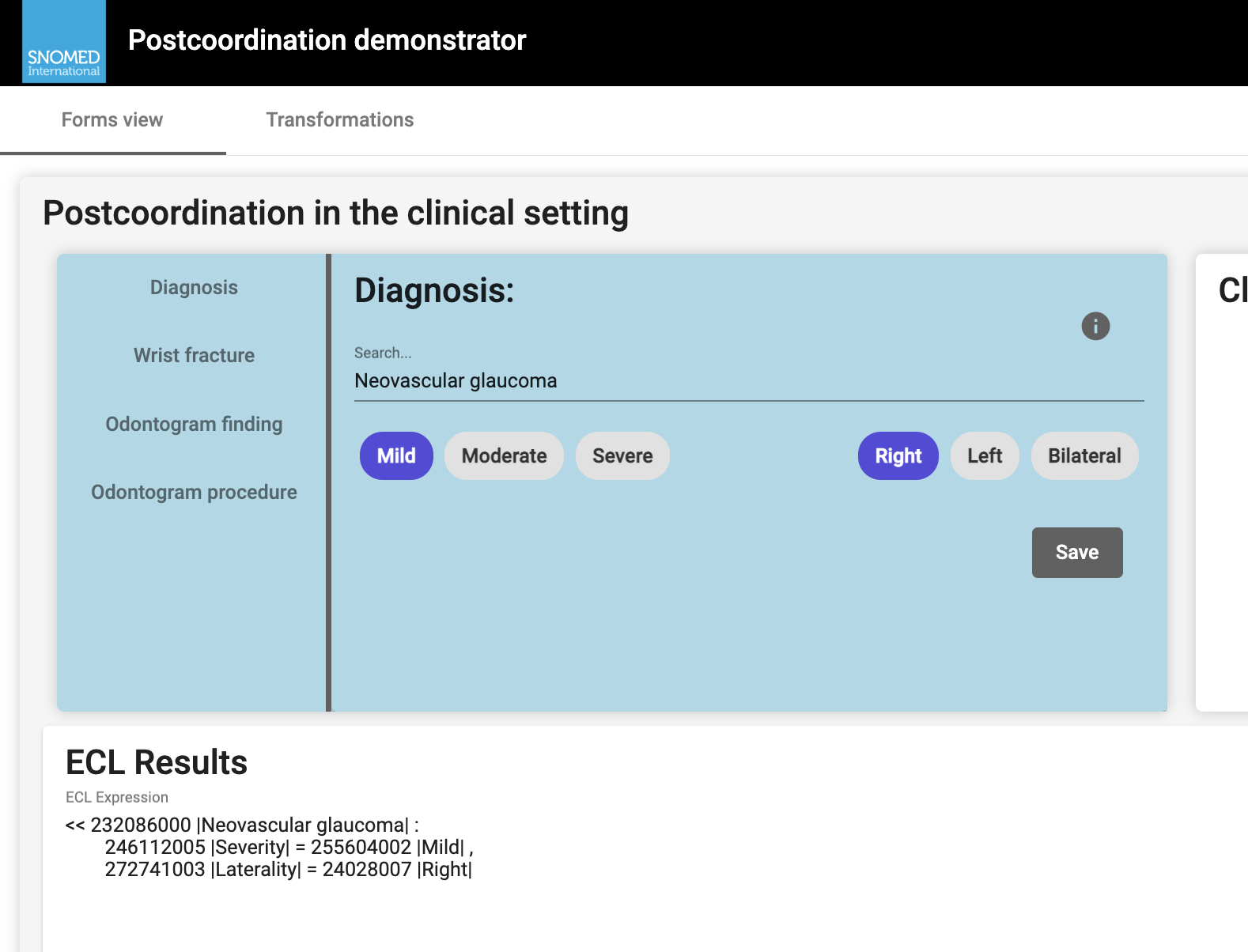
Using postcoordination is challenging, but guidance and tooling are starting to emerge; in the Implementation team and the SNOMED Language Group, we are working on a reference implementation of post-coordination with a demonstrator; you can check that on this demo page:
https://ihtsdo.github.io/iid-postcoordination/
These tools and very early guidance documents will be demonstrated and discussed in the upcoming business meeting. It is still an early time to use these features in production but the demos can show a bit of what might be possible, and how it can present al alternative to creating concepts for all possible combinations.
Best regards
Alejandro